Where we’re Heading in Joint Care: Regeneration, AI Prediction and Evidence Translation

Joint care is on the verge of an evolutionary leap. Innovations in regenerative therapies, data-driven predictive tools and digital health technologies are changing how clinicians approach disease progression, intervention timing and long-term outcomes1. Healthcare providers working in primary care, Musculoskeletal (MSK) services and rehabilitation will need a clear understanding of these developments to support informed clinical decision-making.
Emerging Regenerative Approaches
A number of regenerative and biologically oriented therapies are being explored in joint care, aiming to modulate inflammation and promote tissue repair. The current landscape is summarised below.
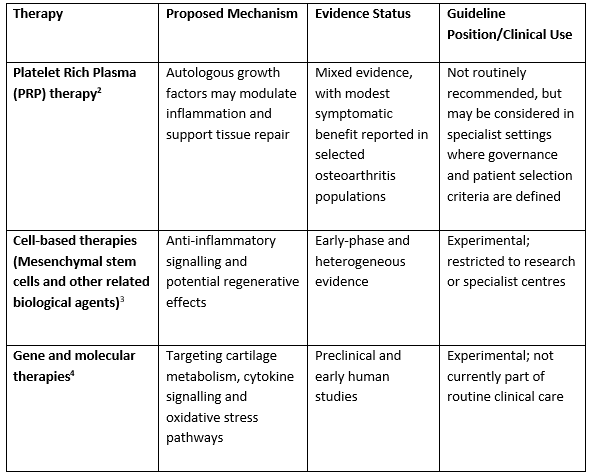
Across current clinical guidelines, regenerative therapies are positioned as adjuncts to established conservative management rather than replacements, with use generally confined to specialist or research settings.

