Complementary and Digital Tools in Joint Rehabilitation: Evidence and Integration

High quality research supports the use of structured exercise,1 weight reduction and maintenance, and education programmes to improve the management of chronic joint conditions, including osteoarthritis (OA).2 These adjunctive strategies can be categorised according to the strength of evidence supporting them:
The important consideration here is that treatment options supportive of rehabilitation should supplement active rehabilitation rather than replace it.
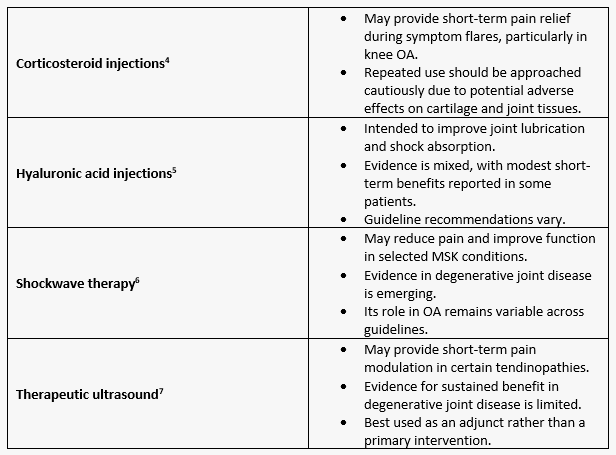
Adjunctive therapies that can support active rehabilitation are typically considered during symptom flares or when pain limits participation in exercise. Understanding their role, limitations and appropriate timing is essential when integrating them into a comprehensive care plan.3

Digital health technologies are increasingly being incorporated into MSK care:8
The current literature indicates that digital health technologies have the greatest potential to improve patient outcomes when utilised within a structured care pathway rather than as independent interventions.
Persistent joint pain is influenced by biological, psychological and social factors. Pain education and cognitive-behavioural strategies help patients understand pain mechanisms, reduce fear of movement and improve self-efficacy for pain management and physical activity. When combined with physical rehabilitation, these approaches can enhance outcomes, particularly in patients with chronic pain or high levels of distress.
The following case examples illustrate how standard rehabilitation approaches can be combined with complementary and digital tools according to patient needs and symptom profiles.
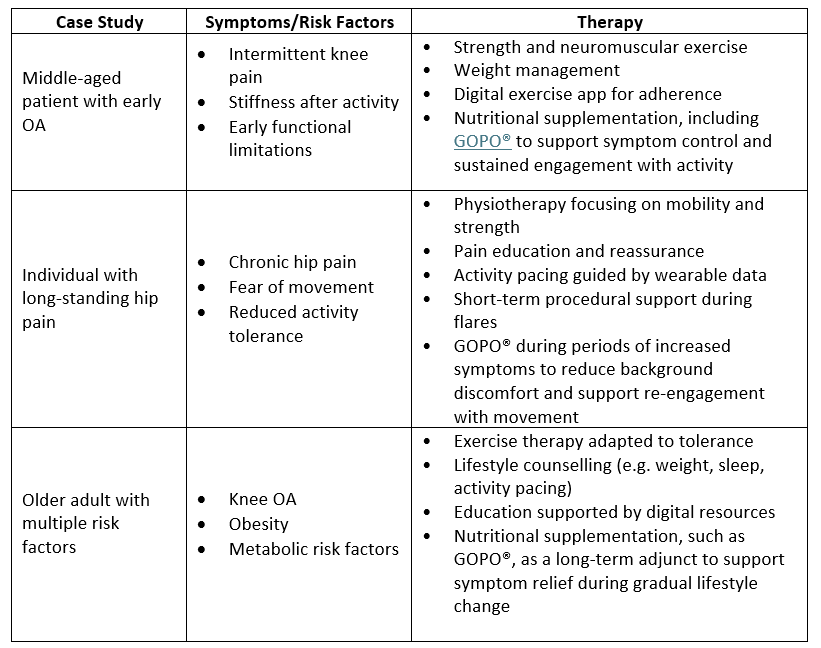
These examples illustrate how adjunctive therapies can be tailored to individual patient needs, preferences and risk profiles within a multimodal care pathway. They also highlight the role of nutritional support as a complementary component of osteoarthritis and joint pain management.
For example, standardised rose-hip formulations12have been investigated in joint health research, with clinical studies reporting improvements in pain, physical function and markers of low-grade inflammation in selected patient populations. Evidence suggests that these benefits are most relevant when nutritional supplementation is used alongside exercise and lifestyle interventions, particularly in patients with early- to moderate-stage disease.13
Critically, healthcare professionals are there to support patients and enable safe evidence-based options by:
The expansion of complementary and digital tools has a growing place in joint rehabilitation when utilised as part of the evidence-based model of care. By combining standard treatments with selected adjunct therapies, healthcare professionals can support personalised, holistic management plans that empower patients, improve adherence and optimise long-term joint health outcomes.
1 Long J, You J, Yang Y. (2025). Effect of Digital Exercise Therapy on the Pain and Physical Function of Patients with Osteoarthritis: Systematic Review and Meta-Analysis. J Med Internet Res.;27:e66037.
2 Cheung THR, Elliott MT, Stephens G, et al. (2025). Effectiveness of digital physiotherapy interventions in patients with knee osteoarthritis: a systematic review and meta-analysis of randomised controlled trials. BMJ Open;15:e102887.
3 French HP, Abbott JH, Galvin R. (2022). Adjunctive therapies in addition to land-based exercise therapy for osteoarthritis of the hip or knee. Cochrane Database of Systematic Reviews, 2022(10), CD011915.
4 Evidence review for the clinical and cost-effectiveness of intra-articular injections for the management of osteoarthritis: Osteoarthritis in over 16s: diagnosis and management: Evidence review J. London: National Institute for Health and Care Excellence (NICE); 2022 Oct. (NICE Guideline, No. 226).
5 McAlindon TE, LaValley MP, Harvey WF, et al. (2017). Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: A randomized clinical trial. JAMA, 317(19), 1967–1975.
6 Liao PC, Chou SH, Shih CL. (2024). A systematic review of shockwave therapy for knee osteoarthritis. J. Orthop. 1:56:18-25.
7 Luo Y, Rahmati M, Kazemi A, et al. (2024). Effects of therapeutic ultrasound in patients with knee osteoarthritis: A systematic review and meta-analysis. Heliyon. 10(10):e30874.
8 Gupta L, Najm A, Kabir K, et al. (2023). Digital health in musculoskeletal care: where are we heading? BMC Musculoskelet Disord 24, 192
9 Paolucci T, Pezzi L, Bressi F, et al. (2024). Exploring ways to improve knee osteoarthritis care: The role of mobile apps in enhancing therapeutic exercise-a systematic review. Digital Health. 10:20552076241297296.
10 Li R, Li Y, Wang L et al. (2025). Wearable Activity Tracker–Based Interventions for Physical Activity, Body Composition, and Physical Function Among Community-Dwelling Older Adults: Systematic Review and Meta-Analysis of Randomized Controlled Trials J Med Internet Res 2025;27:e59507.
11 Thuilier E, Carey J, Dempsey M et al. (2024). Virtual rehabilitation for patients with osteoporosis or other musculoskeletal disorders: a systematic review. Virtual Reality 28, 93.
12 Gruenwald J, Uebelhack R, More MI. (2019). Rosa canina - Rose hip pharmacological ingredients and molecular mechanics counteracting osteoarthritis - A systematic review. Phytomedicine: International Journal of Phytotherapy and Phytopharmacology, 60, 152958.
13 Marstrand K, Warholm L, Pedersen F, et al. (2017). Dose-dependent impact of rose-hip powder in patients suffering from osteoarthritis of the hip and/or knee – a double-blind, randomized, placebo-controlled, parallel group, phase III study. International Journal of Complementary & Alternative Medicine, 7(1), 329–334.
This site is intended for UK healthcare professionals only.